
Psychotherapy and Applied Psychology
Psychotherapy and Applied Psychology is hosted by Dr. Dan Cox, a professor at the University of British Columbia.
This show delivers engaging discussions with the world's foremost research experts for listeners interested in or practicing psychotherapy or counseling to provide expert insights and practical advice into mental health, psychotherapy practice, and clinical training.
This podcast provides valuable insights whether you are interested in psychotherapy, an applied psychology discipline such as clinical psychology, counseling psychology, or school psychology; or a related discipline such as psychiatry, social work, nursing, or marriage and family therapy.
If you want to learn about cutting edge research, improve your psychotherapy/counseling practice, explore innovative therapeutic techniques, or expand your mental health knowledge, you are in the right place.
This show will provide answers to questions like:
*How will technology influence psychotherapy?
*How effective is teletherapy (online psychotherapy) compared to in-person psychotherapy?
*How can psychotherapists better support clients from diverse cultural backgrounds?
*How can we measure client outcomes in psychotherapy?
*What are the latest evidence-based practices?
*What are the implications of attachment on psychotherapy?
*How can therapists modify treatment to a specific client?
*How can we use technology to improve psychotherapy training?
*What are the most critical skills to develop during psychotherapy training?
*How can psychotherapists improve their interpersonal and communication skills?
Psychotherapy and Applied Psychology
Bad Therapy, Better Training, and the Promise of AI
Use Left/Right to seek, Home/End to jump to start or end. Hold shift to jump forward or backward.
Dan responds to listener feedback on topics including AI in psychotherapy, therapy experiences, mental health classification systems, and therapist training. He shares his insights, personal stories, and discusses future directions in mental health practice and research in psychotherapy.
Podcast contact page
https://psychotherapyandappliedpsychology.com/contact.html
HiTOP website
https://www.hitop-system.org/
The Practitioner’s Guide to the Alternative Model for Personality Disorders — Guilford
https://www.guilford.com/books/Practitioners-Guide-Alternative-Model-Personality-Disorders/Bach-Hopwood-Simonsen-Krueger/9781462556489
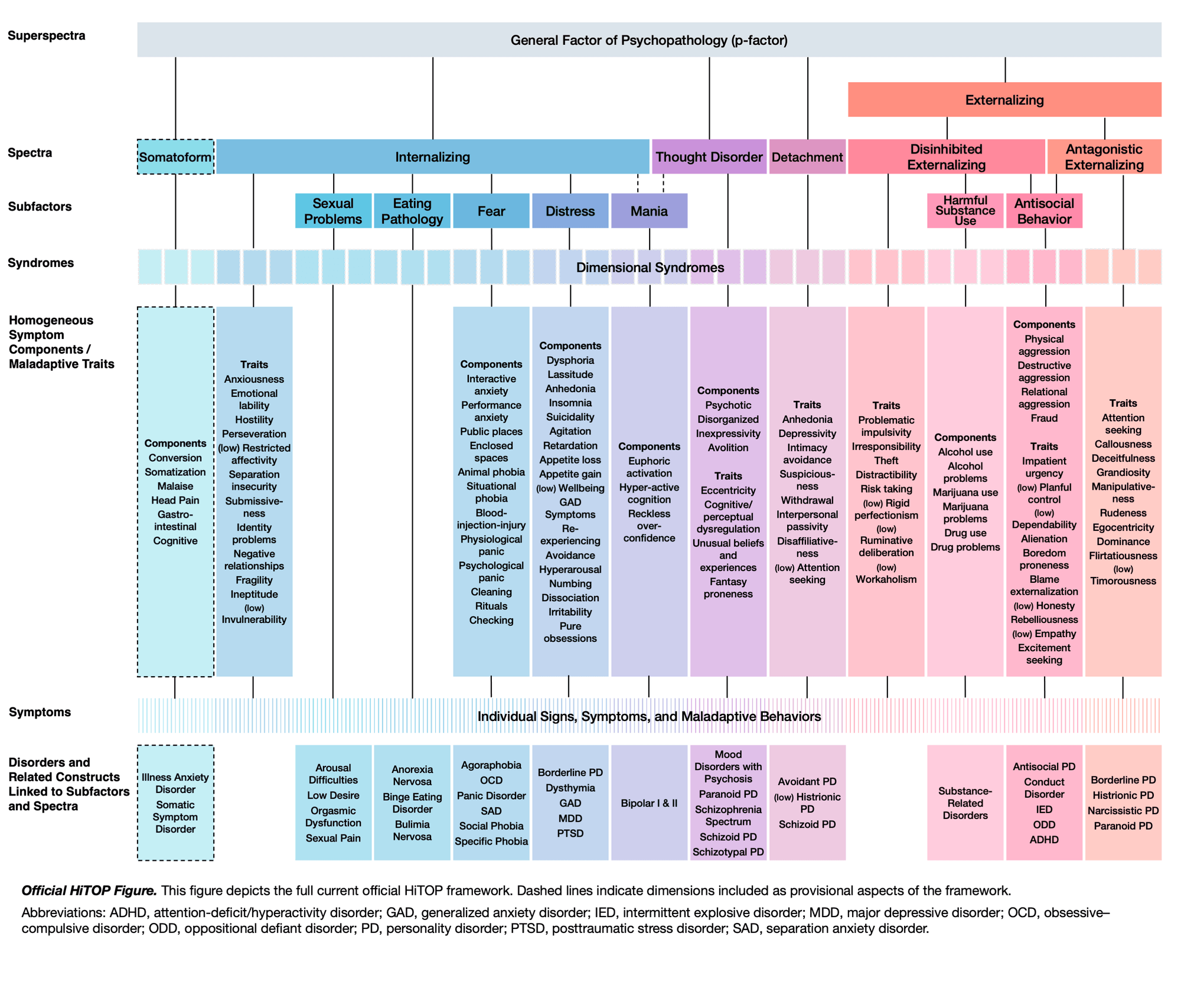
HiTOP in an Image
https://psychotherapyandappliedpsychology.com/pdfs/hitop_model.png
Original HiTOP Manuscript
https://psychotherapyandappliedpsychology.com/pdfs/hitop_manuscript.pdf
Referenced Episodes
Ep 66 : Artificial Intelligence and Mental Health: A New Frontier with Dr. Tony Rousmaniere & Dr. Alexandre Vaz
https://psychotherapyandappliedpsychology.com/ep/17753568-artificial-intelligence-and-mental-health-a-new-frontier-with-dr-tony-rousmaniere-dr-alexandre-vaz.html
Ep 1 : Do therapists get better over time? Discussing therapist expertise with Dr. Terence Tracey
https://psychotherapyandappliedpsychology.com/ep/14809600-do-therapists-get-better-over-time-discussing-therapist-expertise-with-dr-terence-tracey.html
Ep 35 : Therapeutic Alliance Ruptures in Psychotherapy with Dr. Catherine Eubanks
https://psychotherapyandappliedpsychology.com/ep/16460817-therapeutic-alliance-ruptures-in-psychotherapy-with-dr-catherine-eubanks.html
Ep 59 : Revolutionizing Psychiatric Diagnoses: Understanding the HiTOP Model (a DSM Alternative) with Dr. Robert Krueger
https://psychotherapyandappliedpsychology.com/ep/17484719-revolutionizing-psychiatric-diagnoses-understanding-the-hitop-model-a-dsm-alternative-with-dr-robert-krueger.html
Ep 29 : Personality Disorder Diagnosis and Treatment: DSM vs ICD, borderline, and other considerations with Dr. Ueli Kramer
https://psychotherapyandappliedpsychology.com/ep/16159731-personality-disorder-diagnosis-and-treatment-dsm-vs-icd-borderline-and-other-considerations-with-dr-ueli-kramer.html
Ep 55 : How Deliberate Practice is Transforming Therapist Training & Client Outcome with Dr. Tony Rousmaniere
https://psychotherapyandappliedpsychology.com/ep/17342034-how-deliberate-practice-is-transforming-therapist-training-client-outcome-with-dr-tony-rousmaniere.html
Ep 25 : Choosing a Graduate Program in Counselling or Clinical Psychology: What You Need to Know
https://psychotherapyandappliedpsychology.com/ep/15993111-choosing-a-graduate-program-in-counselling-or-clinical-psychology-what-you-need-to-know.html
Ep 72 : Cognitive-Behavioral Therapy (CBT): A Key Player in the Evolution of Psychotherapy with Dr. David Barlow
https://psychotherapyandappliedpsychology.com/ep/17989894-cognitive-behavioral-therapy-cbt-a-key-player-in-the-evolution-of-psychotherapy-with-dr-david-barlow.html
Ep 23 : The Psychology of Perfectionism: The struggle to be good enough with Dr. Paul Hewitt Part 1
https://psychotherapyandappliedpsychology.com/ep/15911724-the-psychology-of-perfectionism-the-struggle-to-be-good-enough-with-dr-paul-hewitt-part-1.html
Ep 66 : Artificial Intelligence and Mental Health: A New Frontier with Dr. Tony Rousmaniere & Dr. Alexandre Vaz
https://psychotherapyandappliedpsychology.com/ep/17753568-artificial-intelligence-and-mental-health-a-new-frontier-with-dr-tony-rousmaniere-dr-alexandre-vaz.html
Ep 15 : Revolutionizing Personality Disorder Diagnosis: Understanding the DSM-5's Alternative Model of Personality Disorders (AMPD) and its Clinical Implications with Dr. Robert Krueger
https://psychotherapyandappliedpsychology.com/ep/15405938-revolutionizing-personality-disorder-diagnosis-understanding-the-dsm-5-s-alternative-model-of-personality-disorders-ampd-and-its-clinical-implications-with-dr-robert-krueger-part-1.html
For more episodes, video versions, updates, and links related to the show visit:
https://psychotherapyandappliedpsychology.com/
[Music] Today we're doing something a little bit different. The first feedback episode of psychotherapy and applied psychology. I've thought about doing this for a while, but I wasn't sure if I had enough feedback. But it turns out that I have more feedback than I'm able to get to. So today I'll be responding to feedback from people coming from the perspectives of clients, patients, family of clients and patients, therapists, students, and prospective students. And for any past episodes that I reference, I'll include links to those episodes in the show notes so that you can easily find the original conversations. My plan is to go for 30 minutes or so, and if this episode isn't a complete disaster, then I'll do another feedback episode in the not too distant future. Also, if you have a question or comment for a future feedback episode, or just because you want to ask me something or let me know something, please send it my way. You can leave a comment on YouTube or you can contact me through the website, which is linked in the show description. I genuinely enjoy hearing what you're thinking about, what you're struggling with, what you disagree with, and what you'd like to hear more about. But first, if you're new here, I'm your host, Dr. Dan Cox, a professor of counseling psychology at the University of British Columbia. Welcome to psychotherapy and applied psychology, where I sit down with leading researchers to pull out practical insights, speak behind the curtain, and hopefully have a little bit of fun along the way. If you're getting value from the show, do me a huge favor and subscribe on your podcast player, or if you're watching on YouTube, hit the like and subscribe buttons. So one of the simplest ways to support the podcast and keep these conversations going. And since this is the first mailback episode, I'll add one more request. If you're listening on Apple Podcasts, Spotify, or whatever podcast player that you use, please do me the world's biggest favor and leave a five star rating. And if you're willing to write a review while you're there, that would be hugely appreciated. It helps other people find the show and it really does make a difference. And onto the first comment. The first comment is about the episode that I did on AI and psychotherapy, although AI and psychotherapies come up a few times since, with Dr. Tony Rumeneer and Dr. Alex Vaz, which I'll link to at Chris2455, wrote, "An LLM is always there when you're most vulnerable and desperately need help. You don't need to wait a week or talk to someone. It's instant support and it can be life changing." So I had a few people write in with sort of similar positive sentiment like that. I also had some people not surprisingly write in with some more negative sentiment. At tomorrow, Forever wrote,"This is what people ignore about AI. They treat it like it's a rational entity. It's not. It's a predictive text generator. Its job is to predict what text should come next. It tries to tell you what you want to hear." So let me just give a few thoughts about this. The first, let me hit on some of the value of AI. Let me tell a little bit of a story. A couple of months ago, my son heard his thumb playing football. And if you're familiar with nine-year-olds, their ability to report what their experience is and how dramatic it is or how not dramatic it is, or how problematic or not problematic it is, their self-reports not so reliable. So you do your best to sort of, and what I did, I did my best to assess,"Okay, how bad is this? It's probably not so bad. He hurts himself all the time playing sports." But then he sort of, it seemed like it wasn't getting better, where over the next day or two, it was still swollen, it was still bruised, he was still complaining in ways that he doesn't normally. So I took a picture of his thumb, threw it into chat GPT, asked a couple of questions, and it was tremendously helpful. And you know, it gives that,"Hey, I'm not a, this isn't professional medical advice. But it also said, "Yeah, this sounds like you should probably go to the doctor's, get it checked out." Next day, we go to the hospital, we get it x-rayed, this thumb is broken. It was a really useful tool. I think for folks who are struggling with some mental health stuff, who are just like, "What am I experiencing? What's going on with me? Should I go and see somebody?" These AI chatbots can be a useful tool for giving folks just someone, or something that has some insight, or potentially some knowledge that could be useful for helping you make these decisions and figure out what's happening. Of course, you have to take it with a huge grain of salt. I've also found that it can be helpful for helping you think things through. Right? I'm feeling really stressed. Let me just sort of talk to this thing, to get to my ideas about how maybe I can handle things better, how I can think through this, or I need to have a difficult conversation with someone. Let's talk to this chatbot. I forgot how to have that difficult conversation. I've just sent a difficult email and I don't know how to word it. All these, I think it can be a really helpful tool, but there are also lots of concerns that need to be considered. We've all heard stories about these tools giving people terrible suggestions, really awful things like to hurt themselves, that life's not worth living, all that sort of stuff. Obviously, that's just the worst. So that's happening in there. I also think we have to be concerned about people using it to play, replace others in a couple of different ways. One is just it's very easy for it to feel like it is an actual other human being and you have an actual real relationship with this sentient entity or conscious entity, which in fact, we don't. I also think we need to be thoughtful about if now I'm starting to go to this machine to get in for to sort of talk things through to process things that I'm probably going to be less likely to talk to my best friend, my mom, my dad, my partner, my whomever, my boss, my coworker, because I can just sort of like process it with this machine. I could ease in many situations. I could see that this is just sort of going to cut off some of those interactions, which help to give you skills to develop those relationships, comfort, disclosing vulnerable stuff to people in your life. There's countless benefits to having these conversations with people and that if we start having more of them with these chat bots, then we're going to have less of them most likely with other people in our lives. I'm the counterpoint is that this might help give us the tools to have these conversations with people in our lives. So, you know, there's the good and the bad of these tools. I think there's going to be a lot that's going to be unfolding over the next couple of years in terms of where this goes. And I'm sure I'll continue to have folks on the podcast to talk about it. But both of these comments along with the many others that I got, I just really appreciate it and I think this is going to be something that's going to be unfolding. And it's important for those of us who are in the mental health research space as well as in the mental health practice space to really be mindful, thoughtful, and consider where these tools are useful and where they're problematic. I've got some feedback also from my episode one with Terry Tracy on therapist expertise. But the comments about bad therapists at, all right, you ready for this one? At me, when if in all together, all the bugs, so that's the handle. It's one word. That's what difficult to read. This person wrote, I got ghosted twice by two different therapists therapy, aimed at the book adult children of emotionally immature parents did more for me than any of my dozen or so therapists combined parenthetical. I have no idea what that book is. Okay, I try to stay away from AI, but it's better than therapists because the bar for being good therapist is low. Then at Nanomka wrote, I was treated at a university training program. The trainees seem more interested in making it look good on paper, or at least not her fault than helping me. Okay, first of all, I'm really sorry that you both and others who wrote in had bad experiences, that sucks. This is how I think about it. I think about therapists like I think about teachers. And the reason why teachers are a useful analogy is we've all had lots and lots of teachers over the years. So we all know there are really great teachers, really terrible teachers, all of the in between. And that it also, you know, for me, I really like this teacher, but for my friend, she hated this teacher. You know, there's a lot of variability there. So that's how I like to think about therapists. It's true for any profession, really, but that's how I think about therapists and how good they are. Unfortunately, there are bad therapists out there. Just straight up, there are bad therapists. We also know that on average, therapy is quite effective. Though all these things are happening simultaneously. So this is the bit of advice that I give to folks who are looking for a therapist or who got a therapist and it didn't go well. One, once you see a therapist, if it's not going well, leave. I encourage people to give it two sessions. But if you go to a first session and you're like, I hate this person, get out of there. If you go to the second session, you're like, I don't, you know, if you're borderline, I would say if possible, go to the third. Just sometimes it just takes a little while. But don't stay in the relationship. If it's not working for you, that's one thing. And instead think, all right, I'm going to sort of date around. So you know, date some therapists. Don't take that literally until I find the one that works for me. So that's what I encourage you to do. If you get one that you don't like, get out of there and also think about like, I'm just going to try. And there's nothing wrong if it's not working just and if possible to even say, hey, I really appreciate this. But you know, I just feel like this isn't what I was looking for or this just isn't working for me. And if you don't feel comfortable, you can always just, you know, bail as well. But I really, again, in the context of we do know that therapy on average is beneficial. We do know that there are therapists who are really great therapists. The evidence for that is extremely clear and that you don't even need the really great therapist to get really effective therapy that you don't give up on it. But instead go and try to find someone who is a better match for you. Okay. A comment in relation to the episode I did on rupture and repair. This was my episode with Dr. Catherine Ubanks at cadman the aviator wrote does rupture and repair presume that there was an alliance. The answer is sort of and there are different ways that people have operationalized therapeutic ruptures or alliance ruptures over the years. So we're doing a study right now where it's a quality. Well, it's a mixed method study, but we're looking at how therapists respond when a client discloses that they're suicidal. And we're particularly interested in sort of what leads to ruptures in those interactions. An example of what this sometimes looks like is when a client discloses suicide. And the therapist then hyperfocuses on the suicide does things like risk assessment or safety planning or something like that. And then the client is they're not very interested in doing what the therapist is trying to do, which is focus on risk assessment and that sort of stuff. So then the client shuts down. So this is one of the things that we're seeing. So that's what we would call an alliance rupture because the client did a what we would call like a withdrawal. So it's a withdrawal rupture because they shut down in response to what the therapist was doing. The other type of rupture at least as conceptualized by Ubanks is rupture resolution rating scale. I think that's what's called the three RS is a confrontation rupture. So this would be imagine the exact same situation. And the client says if this happens, I really don't think life would be worth living anymore. And then the therapist hyperfocuses on the suicide stuff, but the client wants to keep focusing on whatever it is that stress and amount or whatever. And then if the client said, Hey, pay attention to what I'm talking about or why are you talking about that? I don't care about that. Can we focus instead on the pain that I'm going through right now or the difficulties I'm having, not focusing on this other thing that you keep seeing me to focus on. So that would be what we call a confrontation rupture. Both of those that withdrawal rupture or that confrontation rupture, those things could happen in the earliest part of session one. And that would be an alliance rupture. So does there need to be an alliance before you get a rupture sort of, but it's not necessarily how you might think like there needs to be this long developing relationship before you can have a rupture of that relationship. It can happen very quickly. Okay, we had a couple of comments on my episodes with Robert Kruger on the high top model and quick as a reminder, the high top model is the hierarchical taxonomy of psychotherapy at Kowash chic. Go with that asked, is there an, is there any overview book on high top? I did a little bit of research on this. First thing I'm going to point to and I'll link this is there's their website, which is high top h it. It's a great free resource that I encourage folks who are interested in the high top model to go check out. There was also because Kruger was, I think it was almost coming out the last time I own one the podcast, but there's a book that they recently published, which is the practitioners guide to the alternative model for personality disorders, the alternative model for personality disorders is sort of kind of falls within the high top model or akin to the high top model and so I will link that as well in the show notes and then I'll also link a couple of other overview articles of the high top model. There's a lot of resources I couldn't find a book that was really just just the high top model, but there are these other tools and resources that I think will be really helpful for folks are interested also in relation to the high top model. But not my cup of tea wrote this profile dimension narrative of high top made me wonder whether a gold go together with ICF the way DSM goes with ICF I didn't know what the ICF was so I looked it up this is what I got the ICF is a classification framework for describing functioning disability and health related life context over the DSM or ICD might classify disorder these the ICF classifies how a health condition affects someone's functioning in real life is interesting so I don't think and again I'm not an expert on this so maybe I should have somebody on the podcast who knows stuff about the ICF because I know absolutely nothing about it and it sounds very interesting. So a couple of things so I don't think that this would be akin to the ICF like the DSM goes with the ICD because the high top model they developed the high top model solely based on the symptoms from the DSM so that was their you know library of items that they use to develop the high top model. So it's both a strength and the weakness of the high top which is you know it's it uses the exact same symptoms as the DSM so it's really a reorganization of the information that is in or that makes up the disorders in the DSM rather than a separate classification system that's totally autonomous that was developed autonomously it's reliant on the DSM so in that sense. So this is is glued to the DSM but there's something else that I wanted to bring up in response to this comment thinking about the ICF right so this again as I understand it really is a classification system of functioning in real life that I think that what one of the things that's happened over the decades is that the DSM has become experience as like at least in North America I should say and my guess is the ICD in Europe and other parts of the world. But I'll just speak to the DSM in North America because that's what I'm familiar with that it has become the end all be all this is the thing to become reified it's what everyone uses and so you have to work within that framework it's like this framework is the framework how I've come to think about it is the human experience is extremely complicated and so it makes sense that we would have different classification systems for looking at it. In different ways and depending on what the client wants depending on their values depending on their needs the problems they're experiencing as long as as well as from the practitioners perspective what the practitioner finds is useful the framework the practitioner comes from it makes sense to me that we would have different classification systems so that we can look at the human experience in different types of ways one of the real real weaknesses of how it works presently in North America is the DSM in most circumstances is the end all be all and I just don't think that the human experience is that clearly one or two dimensional it's three dimensional so we need to have more ways of thinking about it and looking at it. Following up on the same episode at the Polaris wrote as someone dealing with a loved one with this I would be interested in understanding more about why it changed and the arguments foreign against from moving keeping and changing the board line personality disorder diagnosis. So in relation to the BPD diagnosis one of the things that really stuck with me that Bob Krueger said is when it comes to the DSM what they're doing is they're trying to fix an airplane mid flight so the DSM is out there everybody uses it again at least in North America there's tons of research on that classification system so on those categories in this case on borderline personality disorder so we have to keep and there's also you know there are treatment centers and therapeutic modalities that have been developed with this classification system in mind in particular with borderline in mind they've been developed for borderline so as they change this classification system that will have all sorts of implications for researchers practitioners clients patients family members because it's going to it will impact how we think about these things it makes the treatments that we have if we say oh no this disorder is no longer this thing well now we have to rethink rejig the treatments we have the research we have so it's this we need to repair the airplane without tearing it apart because we're in mid flight and then it's going to crash you know I think it's it's it's kind of stuck between a rock and rock and a hard place because there is this well should we change you know how much should we change the system but we also have to consider what the implications of that will be in the real world for real people so when it comes to the DSM how I'm going to speak more to the DSM in general rather than borderline specifically and what I would say also is so I think we talk a little bit about it I talk a little bit about it with Kruger but also I did an episode which I'll link below with Ulykramer where he's in Europe and I think he was part of some of the the ICD task I'm not sure he was the ICD task force for changing up some of the disorder stuff and so they did a lot of shifts to personality disorders in the ICD and then we talked about that and we talked about borderline and how that has or hasn't changed and why and all this first stuff so go listen to that episode with Ulyk was really insightful and he's really an expert on that stuff but you know I think that the when it comes to the DSM I feel like we can just straight up say that the framework in the DSM is sub optimal and that disorders I hesitate to say all to be that absolutely but most many are sub optimal as well some of them are a little sub optimal some of them are really sub opt and then depending on your perspective you might say this should all be done on a continuum rather than categorically all these disorders so the whole thing stinks but we have decades of research and wisdom so research practice all as a based on this framework so there's just this concern about throwing it out so you know I don't know I don't know I'm really sort of I see the different perspectives and I think it's a challenge and I think that regardless of anything pretty much all of these categories we can say yeah this isn't perfect clearly but what are the implications of changing it okay I also got a couple of comments in relation to my episode on deliberate practice with Tony Rheumeneer at Gabby Hirada 5235 wrote I tried to model deliberate practice into a chat GBT model to drill repetition and procedural memories it's shocking how little we therapist trainees remember from the traditional classroom when we have to perform during sessions and at Alex Thompson 3874 wrote thank you for doing these interviews welcome Alex thank you for saying that it's nice to see therapists who are not particularly in the limelight but are doing important work I've always felt therapy school is missing a lot of the what therapy is a skill I really appreciate these comments and I think you know my experience really is consistent with what these folks are saying which is that a lot of times training programs don't emphasize or facilitate training of skills in the ways that they could or maybe optimally they should so that a little inside baseball you know my program we just recently went through our doctoral level accreditation and we're just going through right now our master's level of accreditation and one of the things that is really striking in going through these processes is that the accrediting bodies they have all these criteria of what you need to do there's very little I mean it's borderline nothing on are you facilitating this sort of skill and skill practice frankly there's there's very little on how can you demonstrate that you're training clinicians who are effective right with any sort of data in any meaningful way the way that you typically show competencies is by having something included in a syllabus in a course so my experience now being on the ground floor of it is that because of these accrediting bodies and their expectations and those expectations really not aligning very much with what these two commenters are commenting on which is are you ensuring that these people can practice and actually do these skills because it's not aligning with that and it pushes programs away from focusing on this sort of skill development one thing I've learned in my life is there's a tendency for people to add stuff to expectations but not take away stuff right so that list of what the competencies are for your training program what's included in whatever that continues to grow over the year but very little gets taken away naturally what happens because the programs need to meet these increasing expectations is that all of it becomes shallower because there's just more right so if I have a five year doctoral program whatever right however you make that whatever that looks like you know it being credit hours whatever that if I have five year doctoral program and the list of what I need to cover in those five years grows and grows and grows then just logically everything gets covered into more shallow level and the expectations are that are increasing are not about showing that your trainees have skills that's not what is being increased so I think that these expectations and really that they don't want to say this I'll say do I say do I say yeah I think that the the changing expectations have very little if anything to do with developing better therapists which sucks and it's very frustrating now the more optimistic side of it is people like Tony and Alex are really leading the way on the deliberate practice approach you're training and you know the deliberate practice is a specific type of approach is it the optimal type of approach I don't know you know there's work being done now we'll find out how quote unquote effective it is in different things but I really appreciate and respect the effort that they're putting into this and they're saying hey we think we have an approach which in our experience helps to train better practitioners and in some of their cases it's helped me become a better practitioner and I've dated proof that or dated to support that and this other stuff then Tony talks about this with accreditation you end up with piles and piles of paperwork and that becomes a big part of the accreditation is the piles of paperwork and we think that we shouldn't be focused on that we need to put front and center training better therapists deliberate practice we think is a way to do that and we're just going hardcore in that direction and that is going to be sort of the altar that we're bowing to and everybody who comes in this program is going to know that this is the focus of the program and we still don't know if this is going to actually create more effective therapists but they're really trying and they're also evaluating it so we will get closer to understanding if it's more effective but I just really respect and appreciate that there are folks who are putting substantial effort into how can we train more effective therapists let's do that so that's the optimistic side so folks are doing that hopefully whether it's deliberate practice or some neighboring framework that this catches on in other programs and maybe even some of the accrediting bodies take notice and this can be done in the past few years and this is going to be a great way to do that and we're going to do that and we're going to do that for the next few years. So, I just want to say that I'm going to do a few more things and I'm going to do some research on how to do that and I'm going to do that. I'm going to do some research on grad school stuff so applying for graduate school, getting into graduate school. So let's talk about a couple of those at Simon Ogyannot, forget it, 6037 wrote, I came from a computer science background and I went and I want to work as a therapist. How do I shortlist programs? Also, is there a way I can find mentors in the field because I come from a non-psychology background and feel completely lost. I want to give you some general thoughts ideas that I typically give to folks who are trying to figure out which program I should go into and particularly if you're coming from outside of the field, then a way to really educate yourself so you're able to make good decisions for you and go into graduates. This is a multi-year commitment so it's worth spending quite a bit of effort on the front end to make sure that you go into the program, the type of program that will really help you get where you want to get because if not, you know, it's a couple of years that doesn't make sense. So anyway, this is what I tell folks. First, figure out what do you want to do, be specific. What do you want to do? What do you want your day to day to look like? Then figure out what are the specific jobs in which specific context that you're interested in working and then talk to people who are doing those things. What you want to do is think, okay, what do I want to do and where do I want to do it? Let me give you some examples for me personally. From a practitioner at lens, I like doing psychotherapy with adults who are relatively high functioning. So what does that mean? So primarily psychotherapy. There are lots of things psychologists do. I'm more interested in the psychotherapy side of things. So that already focuses me, adults again, focuses me. And then the relatively high functioning, and I don't know how exactly to articulate this, but what that really means is I'm not very interested in working with folks with severe mental illness. Your focus, your your folks with notable bipolar disorders gets a frenia, that sort of thing, that's not what I'm into. So that already focuses me quite a bit. A couple other things that I've learned about myself is that I generally don't like working in hospitals. It might be some exceptions to that, but it's a good general rule. And I don't like working inpatient. I've done it a couple of times. It's just not, I just get into the, you know, into the unit numbers like, ah, this is not, it's not where I do well. So I really like working in places when they do some sort of routine outcome monitoring data collection sorts of stuff. So when that sort of assessment is part of the therapeutic process. I really like that. I really like working in places that are innovative when it comes to the challenges that clients are having, having generally speaking per the David Barlow episode that I did. Kind of anything that falls under like the emotional disorders category. I'm good with. So I, you know, using the DSM categorization, which I critiqued earlier, I like working with folks with OCD or generalized anxiety, social anxiety, depression, personality disorders, PTSD, panic, et cetera, et cetera, et cetera. So to me, other than severe mental illness kinds of stuff, any of the emotional disorder stuff, I'm cool with like it does that doesn't matter very much to me. So once you figure out some of that stuff, it really helps you identify. Okay, what are the types or the contexts that I would be interested in working with. And then go talk to those people. That's what you have to do is go talk to those people to figure out what their experience to start get more specific into what I like to work in this place, what I not like to work to this. And then once you're starting to get a sense of that, then you can say, okay, what are the programs that will help me to get in these jobs. A couple of ways you can assess that one, if you go online to the graduate programs, particularly the credit graduate programs, they have to have a list of where their graduates end up working. So that's one way you can figure it out is see where the graduates end up working. The other thing is the people that you're talking to, they are the people who would have a sense of, hey, what are the types of training or the types of programs that will help me get there. So those are some thoughts about picking a good graduate program. Another thing this person asked was about getting a mentor. How do they get a mentor when they're from outside of the field. So one is by talking to these people that I encourage you to talking to that you're getting connected with folks. So that can be where you get some sort of mentorship or develop a mentor. A couple of ways that you can get these connections. One is to work your network. So anybody at all that you know, just say to them, hey, I'm thinking about switching fields. But do you know anybody who does this sort of thing? It is amazing how quickly you will stumble across folks who know other folks who are doing exactly what you want to do. And even if it's adjacent, go talk to them because you might find you're going to learn stuff that's going to impact your decision making in terms of what you might be interested in. And the other way, of course, is to just cold call folks. Obviously this the hit rate for this is not as good as one of their folks within your network. But all you have to do is just, you know, identify folks, email them, call them, whatever it is. And just need to say, hey, I'm really interested in what you do. This is who I am. I'm just thinking about fields or whatever happens to be. Can I have 20 to 30 minutes of your time just to talk to you about it? Another comment that somebody made at Natalie a six years or two asked, would it be a good idea to bring a journal or notebook to an interview? Is one of the pieces of advice that I give people all the time always bring something to write with. You can do it on your phone as a person who talks to people interested in graduate programs and jobs all the time. The phones sort of feel like the person is not paying very much attention. What I encourage you to do, bring something to write with and take some notes while you talk. It doesn't have to be anything substantial. But if you're going to sit down and talk to me or to somebody for 30 minutes or 60 minutes, you're not going to remember it all. Nobody does. So have something to write with to jot some notes. It just shows the person that you're talking to. Hey, I care what you have to say enough that I'm going to write some of it down so I can remember it. Otherwise, the person you're talking to can be left with the feeling of, all right, this person's talking to me just to get something. They're trying to make a connection with me to get something they don't actually care what I'm saying. All right. So I just looked at the time and how long I've been going and I'm going a little bit longer than I thought I would. So I'm going to skip some of these. I'm just going to go to a couple of criticisms that I got when I got more than this. But here are a couple that were in relation to my episode about perfectionism with Dr. Paul Hewitt. These have nothing to do with the content of the conversation, but has XO 14s and wrote get that man a new chair this week is awful great content, marked by the constant sound and then at Sherry D 3299 wrote finally at 14 minute mark they start discussing what perfectionism is up to that point. It was a total waste of time. So thank you for the feedback. Even though it always stings a little bit to get it getting even the critical feedback has been really helpful for myself for my awesome editor Mac to reflect and improve the show. We have we have changed some of our audio editing. I have definitely changed how I have these conversations to try to start them in a more engaging and interesting way. It's always a bit of a challenge, but getting this feedback again while it stings is helpful. So I appreciate it. One more comment from a different episode at Andrea drag in 9074 wrote I understand that you're both acting good faith, but there's lack of structure the conversation starts one point moves briefly to another. It becomes more confusing instead of clear despite the host best efforts to structure it. So I do want to keep these conversations conversational rather than as a lecture you know the first handful of these that I did the way that I sent questions and stuff to the guests. I think they were overly luxury and for those of us who are on the research side of things we give lectures and presentations all the time. So it's very easy for us to fall into that and I don't want that I want these to be more conversational, but I have thought about having primer episodes. People say primer some people say primer. I don't know I say primer. I don't know. Let me know if I should say primer primer primer. I have thought about having primer episodes which are a little bit more lecture like that would go along with the conversational episodes. For an example giving a 20 or 30 minutes structured overview of hewitt's framework for perfectionism or of of alliance ruptures and repairs that would go along with the conversational episodes. I'm not sure if podcast listeners would be interested in something like that or not. If I would just release them on YouTube I have no idea. But anyway, I mean they should just be like five or ten minute overviews. Please let me know I'm sort of doing this in a vacuum getting some feedback. But the more feedback I get the more helpful it is with that in mind let me know how this feedback episode was I feel like it was a little bit bumpy. It's kind of weird because I'm generally a pretty animated person and I'm just looking at a camera and a screen with nobody there. There's nobody to play off of. So maybe if I do another one of these I should have somebody on here to do it with where they're asking me questions. I don't know. But anyway, send me feedback about this feedback episode. Let me know if you want more of it if you want me to do it differently whatever and please send any other feedback on whatever topic ideas, guess suggestions etc that you have. Also, the majority of listeners are from the US and Canada. My next most popular listening locations where people listen from are the United Kingdom, Australia, Germany, New Zealand, Netherlands, Ireland, Italy, followed by South Africa and the list goes from there. Who are you? Drop me a line. I would love to know who you are. How did you find this show? I just see you as a number on my podcast dashboard and the stats is like, oh there's X many listeners from Italy. Who's listening from Italy? That's awesome. I want to hear. I drop me a line. My Irish friends. But you know, there are people from all over the world listening. I would love to just, you know, love to know who you are. It would just absolutely make my day. So please drop me a note, even if you don't think that you have anything to say, just saying hi gives me just the best feelings. And I would appreciate it. So until next time.[Music]

{kind=link}