.jpg)
Drug Safety Matters
Drug Safety Matters brings you the best stories from the world of pharmacovigilance. Through in-depth interviews with our guests, we cover new research and trends, and explore the most pressing issues in medicines safety today. Produced by Uppsala Monitoring Centre, the WHO Collaborating Centre for International Drug Monitoring.
The views and opinions expressed in the podcast are those of the hosts and guests respectively and, unless otherwise stated, do not represent the position of any institution to which they are affiliated.
Drug Safety Matters
#27 When drugs damage the liver – Rita Baião
Use Left/Right to seek, Home/End to jump to start or end. Hold shift to jump forward or backward.
Send a text message to the show!
The liver is the primary site for drug metabolism in the body, but it can be severely damaged by medicines or their toxic compounds. Rita Baião from the North Lisbon University Hospital Center reviews what pharmacovigilance professionals should know about drug-induced liver injury (DILI).
Tune in to find out:
- Who is most at risk of developing DILI
- How to diagnose the condition and control the damage
- How to assess case reports of DILI
Want to know more?
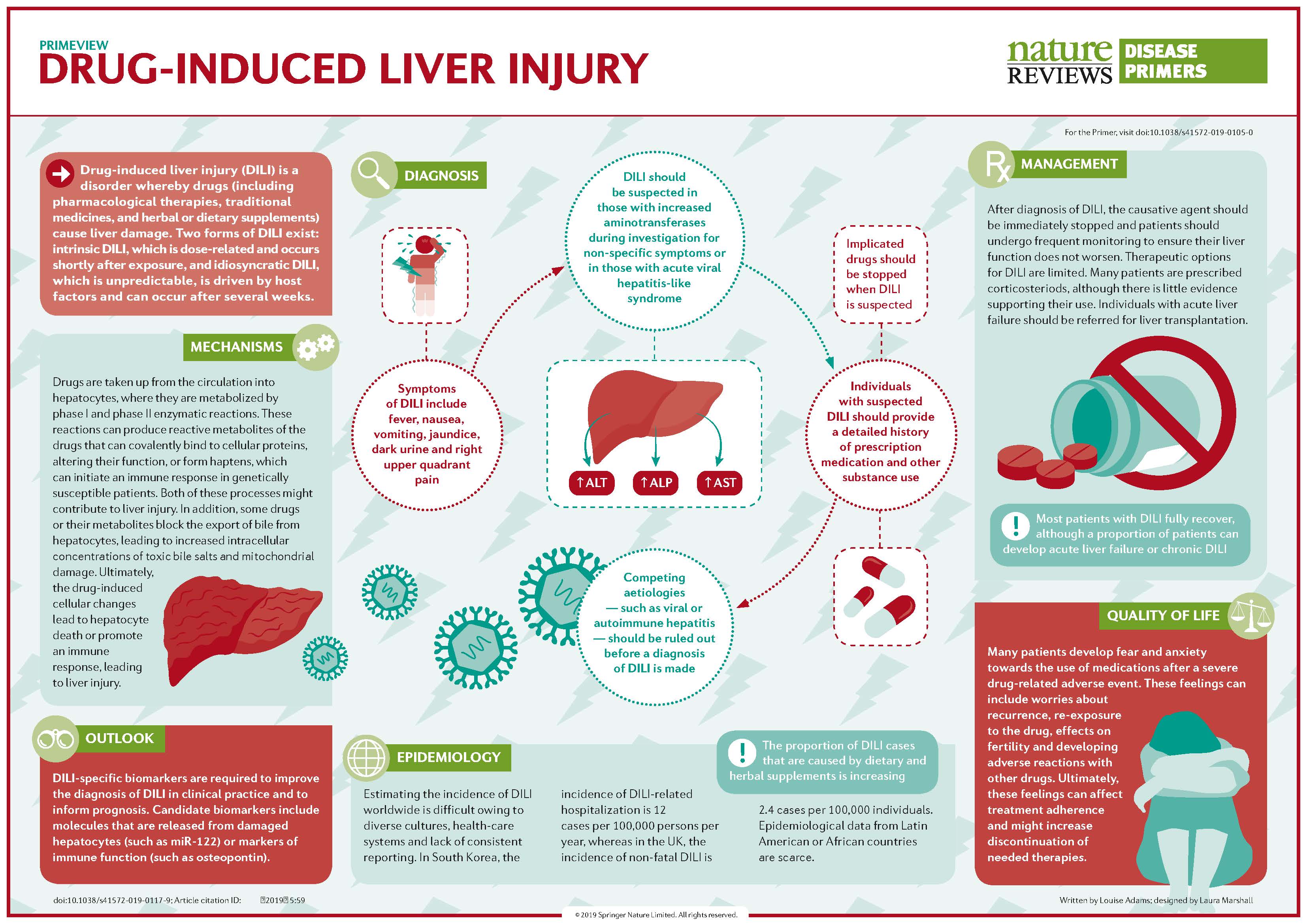
- This infographic in Nature Reviews nicely summarises the mechanisms, diagnosis, and management of drug-induced liver injury.
- In this report, the Council for International Organizations of Medical Sciences provides a global perspective on DILI detection, susceptibility factors, outcomes, and more.
- In this Drug Safety article, industry representatives outline how to identify, mitigate, and communicate the risk of DILI during drug development.
- The PRO-EURO DILI NETWORK coordinates research efforts on DILI across Europe and provides a forum to exchange knowledge and training on the topic. Similar initiatives include the Spanish DILI Registry and the Latin American DILI Network.
- The free online tool LiverTox contains up-to-date information on drug-induced liver injury for medicines and herbal products.
To learn more about post-marketing surveillance and clinical care of DILI, check out Uppsala Monitoring Centre’s free online course on the topic.
For more on the clustering algorithm vigiGroup, revisit this interview with UMC scientists Jim Barrett and Joe Mitchell.
Got a story to share?
We’re always looking for new topics and interesting voices. If you have an idea or any other feedback for the show, get in touch!
About UMC
Uppsala Monitoring Centre promotes safer use of medicines and vaccines for everyone everywhere. Follow us on Facebook, LinkedIn, X, and Bluesky.
Intro
Federica SantoroSooner or later , most of the medicines we take pass through the liver , where they are chemically altered , so the body can easily get rid of them . Normally , this process runs smoothly , but sometimes drugs and their metabolites end up damaging the liver . This condition , known as drug-induced liver injury , can be quite severe for patients and is not that easy to diagnose , so it's crucial that pharmacovigilance professionals are aware of it . My name is Federica Santoro , and this is Drug Safety Matters , a podcast by Uppsala Monitoring Centre , where we explore current issues in pharmacovigilants and patient safety . Joining me today is Rita Baião , medical doctor and clinical pharmacologist from Lisbon , Portugal .
Federica SantoroRita is currently enrolled in a master's programme at the University of Bordeaux , and as part of her thesis , she is collaborating with UMC researchers to explore if VigiGroup , our clustering algorithm , can help detect and assess signals of drug-induced liver injury , and so I seized the opportunity to chat to her while she was in our offices last December . I asked her how drugs damage the liver , who is most at risk , how to cope with the damage, and much more . Enjoy our conversation .
Welcome, Rita!
Federica SantoroHi , Rita , and welcome to Drug Safety Matters . I'm really glad we managed to squeeze this interview in before you leave UMC and head back to Lisbon . How was your time here so far ?
Rita BaiãoThank you , Federica , it has been a really wonderful surprise . Uppsala is a really amazing city . I managed to make a lot of friends here at UMC and also learn a lot , which was the main reason for me to come here .
Federica SantoroLovely to hear that .
Frequency of DILI
Federica SantoroSo today we're talking about a topic that you're especially passionate about: drug-induced liver injury , or DILI for short . We'll probably be referring to it with the acronym mostly from now on . The term is somewhat self-explanatory , as one would imagine . DILI happens when medical products damage the liver , but of course , there's a lot more to it than just that . So why don't we start with this ? How common is DILI ?
Rita BaiãoSo, DILI is actually a rare occurrence in terms of frequency . It is estimated that it can happen from one in each 10,000 people exposed to one in 100,000 people exposed to a drug . Despite this rarity , it is one of the leading causes of drug attrition in drug development, so a lot of drugs in development phase stop because of liver injury . And also it's one of the leading causes of drug warnings by regulatory agencies and even market withdrawals .
Pre- and post-marketing
Federica SantoroThat's interesting and that leads nicely into my second question , actually , because I was going to ask you how relevant DILI is to pharmacovigilance professionals . And so, how many cases are actually spotted already in clinical trials versus picked up in the post-marketing stage ? From what you said , it sounds like both happen , but what's the relative frequency ?
Rita BaiãoSo, we cannot estimate accurately how many happen during clinical trials , because in clinical trials we have a clue because of liver enzymes' elevations and usually the drug is either stopped or the dose is reduced during clinical trials . And then if the drug makes it to approval and then exposed to larger populations , its frequency starts to be more relevant . But we cannot really estimate the actual frequency because for cautionary measures usually the drugs are stopped if the liver enzymes reach a threshold, and so we don't wait for the patient to develop severe symptoms . And so we cannot really estimate a correct frequency , although in post-marketing setting and some registries have shown that , for example in Iceland and in France , that it can be around 14 to 19 over 10,000 people exposed annually .
Federica SantoroI understand that it's tricky , but it's certainly something we want pharmacovigilance professionals to be aware of , right ?
Rita BaiãoExactly . That is why , in post-marketing setting , it's really important that the professionals are aware of this type of injury , because it's tricky to diagnose and also , when it happens , can be really severe
Mechanisms of injury
Rita Baião.
Federica SantoroWe'll get to all that – you mentioned patient registries and the severity and the diagnosis– we'll get to all that in a bit . First , I'd like to talk about mechanism . So, how do drugs actually cause liver injury , and are there certain types of drugs that are more dangerous , so to say , than others ?
Rita BaiãoSo, it's a really complex mechanism that is still being studied , but we can divide in a gross manner drugs that cause liver injury because they are direct agents causing liver toxicity and so they will be dose- dependent , this type of injury,
Rita Baiãowe can kind of predict at which dose the drug will cause liver injury, and those which are independent of the dose and they depend on the host that is receiving the drug , so the patient , and we cannot foresee when it will happen , at which dose it will happen and how severe it will be . And so this type of liver injury , which we call idiosyncratic liver injury , accounts for around 10% of all types of drug- induced liver injury . Usually it is more severe and it's more rare , but when it happens it's something that we really are concerned about because we don't know when the next patient will appear , because we cannot see a pattern in terms of who will have drug- induced liver injury of this type . As for which drugs are more likely to cause drug- induced liver injury , certain types of drugs , such as antibiotics , anti-convulsants , some types of non-steroidal inflammatory drugs , can cause more frequently drug- induced liver injury , although any drug has the potential to cause liver injury because it also depends on the host factors , so in the patient that is receiving the drug .
Risk factors
Federica SantoroRight , and let's talk then about the patient's factors you mentioned . There's a type of DILI where the response is dose- dependent and has more to do with the drug's characteristics , and then there's another type of DILI where it just seems to happen in a bunch of different people with no specific pattern . But surely there must be some risk factors that the community has identified . Who , in your experience , is more likely to suffer from DILI ?
Rita BaiãoSo, the risk factors so far identified are age – so older people are more at risk – those who have moderate to high alcohol consumption , those also that have underlying liver diseases , autoimmune hepatitis, or other types of autoimmune diseases .
Rita BaiãoAlso , we see that pregnant people are more prone to have liver injury although because pregnant people usually don't take so many medicines during pregnancy , we don't see it as frequently . And also people who take many medicines at the same time, so polypharmacy . Then there's genetic predisposition , which has been a field which has developed largely in the last 20 years , and now we know with some type of assurance that some HLA alleles – so, human leukocyte antigen alleles – are connected to liver injury when you take antibiotic drugs such as amoxicillin and clavulanic acid and also flucloxacillin . So , for example , we have a patient that we are kind of sure that has a liver injury that was caused by an antibiotic, but we want to be sure . And if by any chance we have a liver biopsy or we have some type of genetic testing , we can test for these HLA alleles and if they have those in particular , we can be pretty sure that most likely the drugs are the culprits .
Federica SantoroSo you can do that kind of pharmacogenetic screening nowadays .
Rita BaiãoExactly , but it's not in all countries and it's not as routine practice as in other types of diseases , such as oncology , for example .
Federica SantoroAll right ,
Diagnosis
Federica Santoroyou're a medical doctor by training , so you probably can't wait to get into the clinical details of this conversation , and so let's go on to that . How is DILI diagnosed and , more importantly , how do you tell it apart from other conditions that affect the liver ?
Rita BaiãoSo DILI, and why it's so tricky in terms of both the pre-marketing setting as the post-marketing setting, is a really tricky disease to diagnose . It's what we call exclusion diagnosis . So first we have to rule out a lot of different diseases before we can start to say , okay , the medicine was the culprit . And so we have to rule out first what would be most frequent . So viral hepatitis , for example . Biliary obstruction , so for example gallbladder stones or liver cancer that is obstructing the biliary tract . Also alcoholism , because it can be a risk factor but at the same time can also be an alternative diagnosis if we have an exacerbation of alcoholic liver disease . Also autoimmune diseases that can also cause exacerbation of their chronic disease , also can be an exclusion diagnosis . And so we go through it by steps .
Rita BaiãoSo we try to rule out the most frequent ones , which in most countries would be viral hepatitis . Of course , in countries where we know that some types of infections , such as parasites or some types of other virus , we also have to consider those , but mostly viral hepatitis , from A to B to C and also E, hepatitis E, is also an important cause to rule out . And after that then we start considering okay , maybe the drug was the culprit , but we don't usually wait for confirmation of other diagnosis before stopping the drug . So if there's even a slight suspicion of drug- induced liver injury , most of the drugs – unle ss essential ones which assure life maintenance – we stop all of them . To protect the patient . Exactly .
Controlling the damage
Federica SantoroRight , and is there anything you can do to reverse the damage once some has occurred ?
Rita BaiãoSo, there's no antidote for liver injury . What we can do is removing the suspect drug that can be the culprit . So maintenance therapy , so supporting symptoms . For example , lots of patients develop jaundice and so they get pruritus , and so we give them antihistamine drugs or other drugs that are off-label to support with the pruritus, that can be really disturbing for some patients . And also , for example , if they de veloped coagulation issues , we monitor coagulation v alues to see if we need to start some type of therapy to prevent hemorrhage . The only drug that has an antidote for liver injury is paracetamol or acetaminophen , which is N- acetylcysteine . And so if we have , for example , intoxication by paracetamol in high doses , one antidote that is usually given N-acetylcysteine , but it's an antidote that it's a bit controversial and not all clinicians agree on , but it's the only antidote that we have for drug-induced liver injury , but it's only for that specific
Impact on adherence
Rita Baiãodrug .
Federica SantoroI'm also thinking this is a particularly important adverse event . I mean, it's potentially life-threatening and how does that affect patients' feelings about medicines in general ? I imagine it can be difficult for someone who experiences an adverse event of that severity to take medicines again after that . Is that something you think about ?
Rita BaiãoYes , so definitely , patients become reluctant of taking the same drug , even if afterwards you actually rule out that the drug, so even if you find an alternative diagnosis that was actually most likely to begin with, since you've told them that might be the drugs and you actually stopped the drugs for a while they might still be reluctant to take drugs . And so you really have to be patient and explain that there is also a benefit–risk assessment . And with the patient , you have to also respect their choices , of course , and try to make them understand that , yes , it could have been the drug . If it was the case , then the medication has to be changed . But if it wasn't the drug , we need to rebuild the trust on the therapy .
Rita BaiãoThere's also the opposite , actually . So there are some cases in which we know that some type of medicine causes drug-induced liver injury , but because these medicines are life-saving and they are the only therapeutic option for some diseases , patients really cling on to them . And so , even if the doctor or health care professional says, 'we need to stop this drug because it's damaging your liver' , the patients say, 'but this medicine makes my life better and so I'd rather risk it and have a comfortable day-to-day life or (at least if it's , for example , oncology drugs) I still want to have a chance' . And that can be a bit conflicting , because you don't want to remove their chance of a better life but at the same time you know that the medicine is hurting the liver and damaging the liver . So it can be tricky and it's a patient and doctor relationship that has to be built to regain the trust of the patient .
Federica SantoroYeah , I understand , and that's when it's so important to have those really frank and clear conversations on the benefits and risks , as you say , so that the patients can make the best informed decision they can .
Rita BaiãoThere's also , there's a case that is actually not that long ago with a medicine .
Rita BaiãoThis is public knowledge . So, it was a drug that was used for uterine fibroids , for women with the symptoms of uterine fibroids who'd had menstrual cramps , hemorrhages , very frequently . And the drug was introduced in 2012 in the European market and then by 2017 , some cases had accumulated of liver transplant . And so , of course , a drug-induced liver injury very severe, enough severe for the patients to need a liver transplant , and then the recommendation of regulatory agencies at first would be to remove the drug from the market because this was too severe . But then , at the same time , there was no alternative for these women to treat their symptoms of their daily life , so they had to live with the amaryngis and anemia from their day-to-day life , and removing this drug from the market for them was not an option , because this was a drug that was used for women who could not undergo surgery for uterine fibroids . And so it's a case where it doesn't happen what you expect it to be , which would be patients advocating for the drug to be removed from the market .
Federica SantoroExactly, one of those cases where the regulators think they're taking the best decision for the patients , but actually the patients want something else .
Rita BaiãoYeah , now it's restricted, now there's heavy liver monitoring . But so there is this option and now there are more options , but now it's restricted but not withdrawn from the market .
Analysing DILI reports
Federica SantoroLet's give some practical advice to our fellow pharmacovigilance colleagues who are listening in . When they are analysing case reports for DILI, is there anything special they should do or look out for ?
Rita BaiãoSo, I'd say the most important thing would be to do what you usually do in pharmacovigilance , which is make a calendar or make a graph of exposure: start and stop dates and time to onset or time from cessation of the drug . That's a rule for all pharmacovigilance causality assessment and it's no different for drug- induced liver injury . Here the difference is there are some causality assessment tools that are very specific for liver injury , aside from the general ones that we already know , like the WHO- UMC causality assessment tool . And so there is a very popular one which was invented and developed in the late 80s , which is the RUCAM scale or Roussel Uclaf Causality Assessment Method , and that very recently was updated by a team of experts to RECAM scale . So these are other tools that are very liver- specific to do causality assessment .
Rita BaiãoOf course , the basic rules of causality assessment for other types of drugs still apply . So, exclusion of other causes is very important since DILI is an an exclusion diagnosis . Time to onset, course of action after de- challenge, and when re-challenge is conducted , which is risky in case of DILI, how does the re-challenge occur ?
Federica SantoroAnd so , in addition to those criteria that are included in standard causality assessment methods , do these DILI- specific methods include then other parameters ?
Rita BaiãoIt's a score method and so you point , but it's mostly a guidance , so you don't need to be attached to the score to decide the probability . Of course the score points to a possible , probable, or unlikely causality , but in the end you can decide for yourself , and it helps you do a mental process of thinking, 'is this drug the culprit or not' ? And so it has some parameters that are liver- specific , such as, 'which diagnosis have you excluded so far' ?
Federica SantoroOkay , so guided thinking . Exactly
Patient registries
Federica Santoro. Another way we can learn about DILI , aside from spontaneous reporting systems , is through patient registries , and you mentioned them at the start of the interview . I'd like to go back to that , because back in Portugal , where you're normally based , you're involved with one such registry , the PRO-EURO DILI NETWORK . How does that work ?
Rita BaiãoSo fortunately , and I'm very thankful to have been incorporated by some colleagues back in Lisbon into this network . This network is a European consortium of hospitals throughout Europe which collaborate in gathering evidence for liver disease . And so it's a prospective observational study in which the patients that arrive to our hospitals, be it through the emergency room or consultations/ appointments, and if we suspect they have drug- induced liver injury , we ask them, 'would you like to participate in this study ? ' . And so we get the informed consent , and if they do consent , we gather clinical data , so we make an interview to ask them, 'how have you been feeling ? ', their symptoms . We also collect laboratory assessments . So if they are going to do laboratory assessments , we gather extra blood tubes , and so we try to avoid getting extra laboratory assessments , because that can be uncomfortable for the patients .
Rita BaiãoAnd if their liver disease progresses and by some chance they do have to do a liver biopsy , we also keep a piece for the biobank . And so this is stored in a biobank , and then their cases are presented within a Delphi panel of hepatologists and experts which decide if the case is most likely DILI or most likely a control . And a control doesn't mean that they don't have liver disease , just means that they have other types of liver diseases . If we don't have enough information to decide whether it's DILI or a control , the patient is excluded from the study and then we can compare how DILI differentiates itself from other liver diseases and we get clues from the biological samples of what difference we can see in this type of liver injury . And it's really interesting .
Federica SantoroAre there more networks like this around the world ?
Rita BaiãoYes , so the PRO-EURO DILI started out . Before there was the Spanish DILI registry , which still exists , and then PRO-EURO DILI developed into a European effort . And there's also the North American . Maybe there are more that I'm not aware of , but at least these two are two big ones that are known and are doing really great work in trying to understand DILI .
Federica SantoroAnd we'll link to them in the show notes , along with other resources , so if people are interested , they can read up .
Clustering DILI reports with vigiGroup
Federica SantoroSo, lately though , as we said , you took a break from your usual work in Lisbon and spent some time here at UMC as a visiting scientist . What did you research then in the last few months ?
Rita BaiãoSo, my current research focuses on using a method that was developed here at UMC, vigiGroup , which is a clustering method to aggregate reports based on the co-reported adverse drug reactions that they have inside . And my research is trying to see if , using this method , we can find DILI or if we can build a case series that is clinically coherent . And so we've been focusing more on this latter part , because this is an extensive work and to find new DILI signals we still need to do a bit more research . But for now what we're doing is trying to see if with known drugs , drugs that have been known for the past, I don't know, 40- 50 years, those that we are very comfortable with their safety profile, we can see the patterns of DILI in their clusters that we get from vigiGroup . And we compare , for example , drugs that we know are pretty safe for the liver , so drugs not usually associated with DILI , and we compare their clusters with drugs that we know that cause DILI .
Rita BaiãoAnd so we're trying to see if the patterns of clusters are very distinct . And so we're using a positive and a negative control , and if , within the clusters of drugs that are associated with DILI , if the clusters are clinically coherent – and so if the adverse drug reaction terms that we find within the clusters make sense together . And we'll see the results . We hopefully will have positive results , but we still have to work a little bit more on this . Hopefully it will be useful at least for case management , so for signal assessors to have a case series that is more specific and more manageable in terms of human resources and time .
Benefits of vigiGroup
Federica SantoroWe have an episode on vigiGroup in our archive , so people can listen to that if they'd like to know more about the method . But for those who haven't listened to it yet , can you explain briefly what the advantage is , then , of using a clustering algorithm compared to traditional pharmacovigilance methods ?
Rita BaiãoAnd so this clustering method will aggregate reports . So usually we start with disproportionality analysis and then we build a case series based on the adverse drug reaction that we found was disproportional . But sometimes countries or reporters have different reporting practices and so , for example , if a patient has a drug- induced liver injury , they will complain of jaundice or yellow eyes or pruritus . But if it's the doctor that is reporting the same adverse drug reaction , he will report hepatitis or colostatic liver injury . Maybe if it's a pharmaceutical industry , they will report liver enzymes abnormal or increased . And so with vigiGroup , based on the co-reported terms , we're trying to see if we can group the reports that make sense together and this can build case series that are more coherent . And so for signal assessors and for signal management it's much more directed than just using Standardised MedDRA Queries that sometimes can be too broad .
Federica SantoroAnd again , for those who want to know more , go dig in the archive . We'll link to the vigiGroup episode in the show notes as well . Well , that was all I had for you , Rita , today . Thank you very much for taking the time to join me . I wish you all the best in wrapping up your research here , and we look forward to seeing the results when available .
Rita BaiãoThank you , Federica , and thank you for having me here at UMC .
Outro
Federica SantoroThat's all for now , but we'll be back soon with more conversations on medicines safety . If you'd like to know more about drug-induced liver injury , check out the episode show notes for useful links . If you like our podcast , subscribe to it in your favourite player so you won't miss an episode , and spread the word on social media so other listeners can find us . Apart from these in-depth conversations with experts , we host a series called Uppsala Reports Long Reads , a selection of audio stories from UMC's pharmacovigilance news site , so do check that out, too . Uppsala Monitoring Centre is on Facebook , LinkedIn and X , and we'd love to hear from you . Send us comments or suggestions for the show or send in questions for our guests next time we open up for that . For Drug Safety Matters, I'm Federica Santoro . I'd like to thank Rita Baião for her time , Matthew Barwick for post-production support, and of course you for tuning in . Till next time .



{kind=link}
Podcasts we love
Check out these other fine podcasts recommended by us, not an algorithm.

ECDC: On Air
European Centre for Disease Prevention and Control
Inside EMA
European Medicines Agency
LSHTM Viral
LSHTM